
Breast Cancer LN Status app for iPhone and iPad
Developer: diepflap.it Medical Software
First release : 11 Feb 2013
App size: 8.02 Mb
According to current protocols, sentinel lymph node biopsy remains the gold standard, and in this perspective, a preoperative statistical tool can be useful to communicate to the patient the probability that it will be positive. The future goal of the application of the models presented is to avoid sentinel lymph node biopsy in low-risk patients and avoid completion axillary lymph node dissection in patients with positive sentinel lymph node
Risk of Lymph Node Metastasis Tool
In the univariate analysis, all the risk factors considered (Age, Grading, Tumor Size, LVI, Multifocality, Molecular Subtype) are significantly associated with the occurrence of metastatic lymph nodes. In the multivariate analysis, all the significant variables in the univariate were included. A nomogram was developed with the predictors of the multivariate model to calculate a score for the probability of metastatic sentinel lymph nodes.
Risk of >3 Lymph Node Metastasis Tool
In addition to assessing the risk of occurrence of metastatic lymph nodes, an in-depth study was carried out to evaluate the risk of having more than 3 metastatic lymph nodes (equivalent to the pN2a stage), due to the therapeutic implication in this finding. In patients with more than 3 metastatic lymph nodes, in fact, the Radiotherapy of the axillary and supraclavicular lymph node stations is indicated.
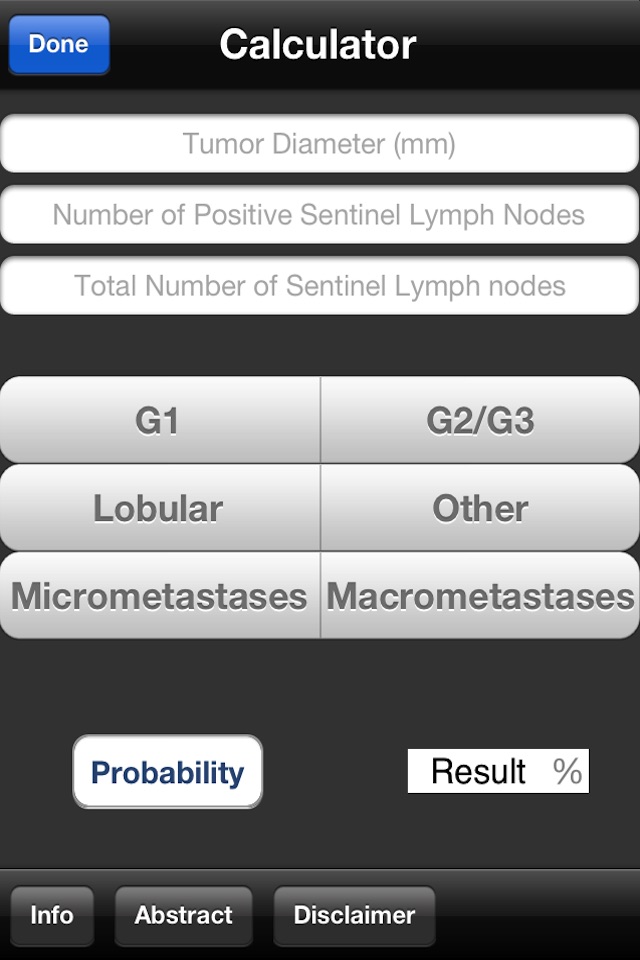
Risk of Non-Sentinel Node Metastasis
Discordance of intraoperative analysis with definitive histology of the sentinel lymph node in breast cancer leads to completion axillary lymph node dissection, which only in 35-50% shows additional nodal metastases. A nomogram was developed to calculate a score for the probability of Non-sentinel lymph node metastases in breast cancer patients with a positive sentinel lymph node.
WARNING:
All tools must not be considered as an alternative but as a complement tool to the experience and ability of the surgeon in the decisional process of treating breast cancer patients.